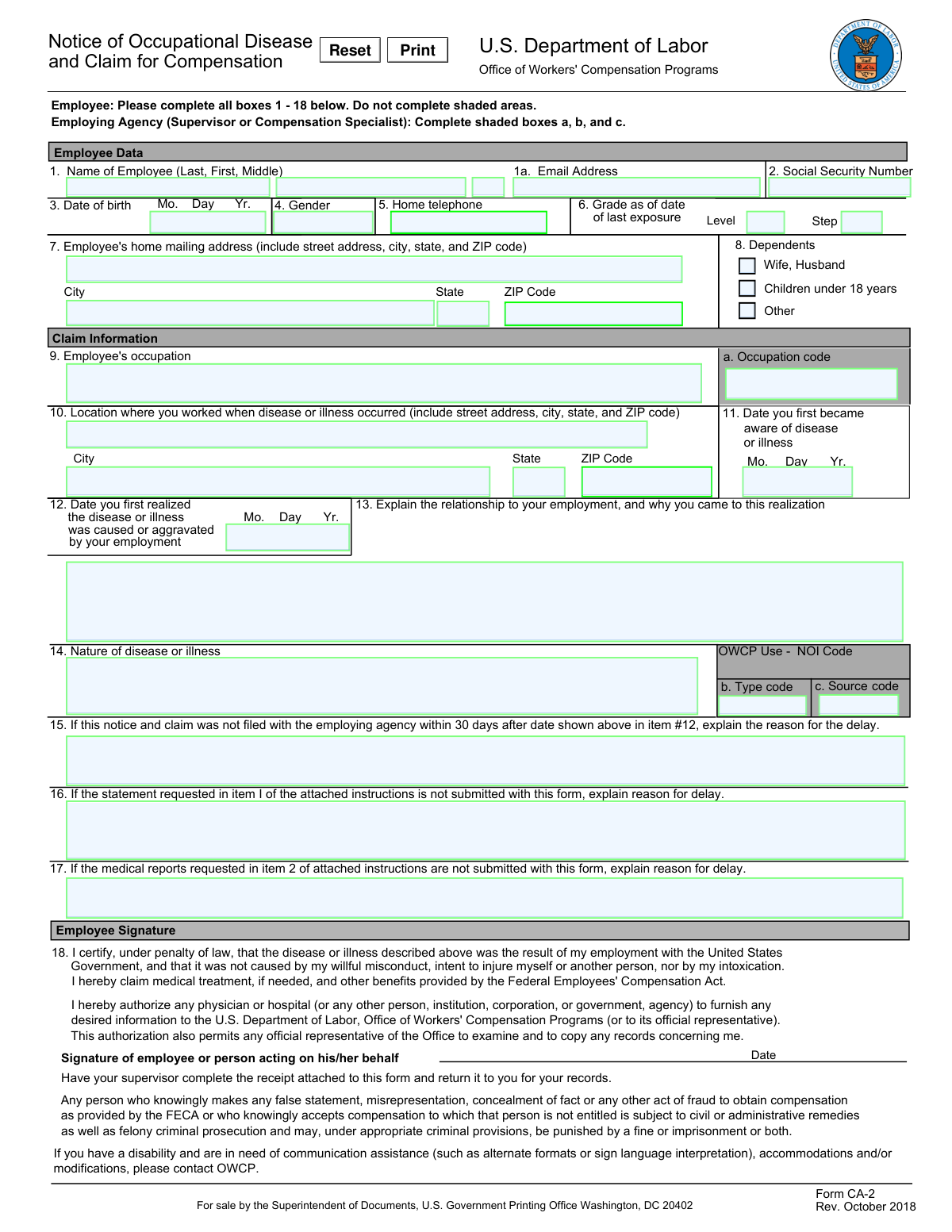
It is essential to provide the full name of the employee, including the last name, first name, and any middle names or initials. Failure to do so may result in processing delays or potential rejection of the form. To avoid this mistake, ensure that all name fields are completely filled out with accurate information.
Entering an incorrect Social Security Number can lead to significant issues, such as delayed or incorrect processing of the claim. Double-check the number entered against the employee's Social Security card or other official documentation to ensure accuracy. Additionally, be cautious when manually entering numbers to avoid transposition errors.
Providing an incomplete or incorrect date of birth can cause processing delays or potential rejection of the form. Ensure that all fields, including month, day, and year, are filled out accurately. Double-check the information against the employee's official documentation to ensure its correctness.
Indicating an incorrect gender in Item 4 can lead to processing delays or potential rejection of the form. Ensure that the gender field is filled out accurately based on the employee's identification documents. Double-check the information to avoid any potential errors.
Leaving the home telephone number blank in Item 5 may cause processing delays or potential rejection of the form. Providing a valid home telephone number is crucial for effective communication between the employer and the employee regarding the claim process. Ensure that the number is entered correctly and is complete with area code and phone number.
When completing the Notice of Occupational Disease and Claim form, it is essential to provide accurate information in Item 6 regarding the grade and step/level. Incorrect entries may lead to processing delays or potential denial of benefits. To avoid this mistake, double-check the payroll records or consult with the employer's human resources department to ensure the correct information is provided.
Providing an incomplete or incorrect home mailing address in Item 7 may cause delays in receiving important correspondence and forms related to the claim. To prevent this mistake, ensure that the address provided is complete, including the street address, city, state, and zip code.
Failing to list all dependents in Item 8 may result in the claim being underpaid or denied. It is crucial to include all dependents to ensure that the family receives the full benefits to which they are entitled. To avoid this mistake, carefully review the list of dependents and include all individuals who meet the eligibility requirements.
Leaving the occupation blank in Item 9 may cause processing delays or potential denial of the claim. Providing an accurate occupation is necessary to determine eligibility for benefits. To prevent this mistake, ensure that the occupation is clearly stated, including any job title or description.
Providing an incomplete or incorrect location where the disease or illness occurred in Item 10 may lead to processing delays or potential denial of the claim. It is essential to provide the precise location, including the address, city, state, and zip code, to enable a thorough investigation of the claim. To avoid this mistake, double-check the location details and consult with the employer or healthcare provider if necessary.
One of the most common errors on the Notice of Occupational Disease and Claim form is entering an incorrect date in Item 11. This field requires the exact date when the employee first became aware, or had reason to believe, that they had contracted the disease or illness. Incorrectly recording this date can delay the processing of the claim and potentially result in a denial. To avoid this mistake, double-check the date with the employee's records and ensure it is accurately recorded.
Another frequent error on the Notice of Occupational Disease and Claim form is entering an incorrect date in Item 12. This field requires the exact date when the employee first realized, or should have realized, that their disease or illness was caused or aggravated by their employment. Incorrectly recording this date can also delay the processing of the claim and potentially result in a denial. To avoid this mistake, consult the employee's medical records and discuss the timeline of their symptoms and employment history.
A common oversight on the Notice of Occupational Disease and Claim form is neglecting to provide a clear explanation of the relationship between the disease or illness and the employment in Item 13. This field requires a detailed description of how the employment contributed to the development or aggravation of the disease or illness. Failing to provide this information can result in a denial of the claim. To avoid this mistake, gather all relevant information about the employee's job duties, working conditions, and any other factors that may have contributed to the disease or illness.
Another common mistake on the Notice of Occupational Disease and Claim form is failing to provide a clear and detailed description of the disease or illness in Item 14. This field requires a thorough explanation of the nature and cause of the disease or illness, as well as any symptoms the employee is experiencing. Leaving this field blank can result in a denial of the claim. To avoid this mistake, consult the employee's medical records and discuss their symptoms and diagnosis in detail.
A less frequent but still important mistake on the Notice of Occupational Disease and Claim form is failing to provide a valid reason for the delay in filing the notice and claim within 30 days in Item 15. This field requires a detailed explanation of any circumstances that prevented the employee from filing the notice and claim within the required timeframe. Failing to provide this information can result in a denial of the claim. To avoid this mistake, document any reasons for the delay, such as extended hospitalization or lack of awareness of the requirement, and provide this information when filing the claim.
The Notice of Occupational Disease and Claim form requires the reason for any delay in submitting the statement requested in Item 1 to be explained in Item 16. Neglecting to provide this explanation can lead to processing delays or potential denial of the claim. To avoid this mistake, ensure that you provide a clear and concise explanation for any delays in submitting the statement as soon as possible. This information is crucial for the processing of the claim and helps to maintain an accurate record of the occupational disease and related events.
Item 2 of the attached instructions requests that medical reports be submitted with the form. Neglecting to include these reports can result in the claim being incomplete and potentially delayed or denied. To prevent this mistake, make sure that all required medical reports are gathered and included with the form when it is submitted. This will help to ensure that the claim is processed efficiently and accurately.
Certifying the claim by signing and dating the form in Item 18 for the Employee Section is a crucial step in the process. Failing to do so can result in the claim being considered incomplete and potentially delayed or denied. To avoid this mistake, carefully review the information provided on the form and ensure that all required signatures and dates are obtained and included before submitting the form.
The Notice of Occupational Disease and Claim form requires the occupation code to be entered in Box a for the Employing Agency Section. Neglecting to provide this information can lead to processing delays or potential denial of the claim. To prevent this mistake, make sure that the correct occupation code is entered in the designated box before submitting the form. This information is essential for the processing of the claim and helps to ensure that the claim is classified correctly.
Item 1 of the attached instructions requests that the type code be entered in Box b for the Employing Agency Section. Failing to provide this information can result in the claim being incomplete and potentially delayed or denied. To prevent this mistake, make sure that the correct type code is entered in the designated box before submitting the form. This information is crucial for the processing of the claim and helps to ensure that the claim is classified correctly and that the appropriate benefits are paid.
The Notice of Occupational Disease and Claim form requires the source code to be indicated in Box c for the Employing Agency Section. This code is essential for identifying the specific statutory provision under which the claim is being made. Failure to provide this information may result in processing delays or potential rejection of the claim. To avoid this mistake, ensure you have the correct source code before filling out the form and double-check that it has been entered correctly in the designated box.
Item 23 of the Notice of Occupational Disease and Claim form requires the name and address of the physician who first provided medical care to the employee. This information is crucial for the processing of the claim and may be required for further communication with the physician regarding the employee's condition. Failure to provide this information may result in processing delays or potential rejection of the claim. To avoid this mistake, ensure you have the correct name and address of the treating physician before filling out the form and double-check that it has been entered correctly in the designated fields.
Item 24 of the Notice of Occupational Disease and Claim form requires the first date medical care was received to be indicated. This date is important for determining the timeline of the employee's condition and the potential eligibility for benefits. Failure to provide this information may result in processing delays or potential rejection of the claim. To avoid this mistake, ensure you have the correct date of the first medical appointment before filling out the form and double-check that it has been entered correctly in the designated field.
Item 25 of the Notice of Occupational Disease and Claim form requires the claimant to answer whether medical reports show the employee is disabled for work. This information is essential for determining the employee's eligibility for benefits and the potential need for further investigation. Failure to answer this question may result in processing delays or potential rejection of the claim. To avoid this mistake, carefully review the medical reports and determine whether they indicate the employee is disabled for work before filling out the form and double-check that the answer has been entered correctly in the designated field.
The Notice of Occupational Disease and Claim form may require additional evidence or information to support the claim. This may include, but is not limited to, medical records, witness statements, or documentation of lost wages. Failure to provide this information may result in processing delays or potential rejection of the claim. To avoid this mistake, carefully review the instructions on the form and gather all necessary documentation before filling it out. Ensure that all required documents have been attached or included in the submission.
Upon submission of the Notice of Occupational Disease and Claim form, it is essential to ensure that the employee receives a copy of the Receipt of Notice of Disease or Illness. This receipt serves as proof that the claim has been filed and acknowledges the employee's right to file for compensation. Neglecting to provide this receipt may lead to confusion and potential delays in the claims process. To avoid this mistake, make sure to keep a copy of the receipt for your records and provide a copy to the employee as soon as possible after filing the form.
The Notice of Occupational Disease and Claim form contains a Privacy Act statement that outlines how the employee's personal information will be used during the claims process. Failing to review this statement carefully may result in misunderstandings about how the information will be handled. It is crucial to understand the implications of sharing personal information and ensure that all necessary precautions are taken to protect the employee's privacy. To avoid this mistake, take the time to read and understand the Privacy Act statement before submitting the form.
In Item 1a of the Notice of Occupational Disease and Claim form, there is a section for the employee to provide an email address for non-case specific communication from the OWCP. Failing to provide this information may result in important updates and notifications being missed. It is essential to ensure that the email address provided is accurate and up-to-date to maintain effective communication throughout the claims process. To avoid this mistake, double-check that the email address provided is correct and encourage employees to update their contact information as needed.