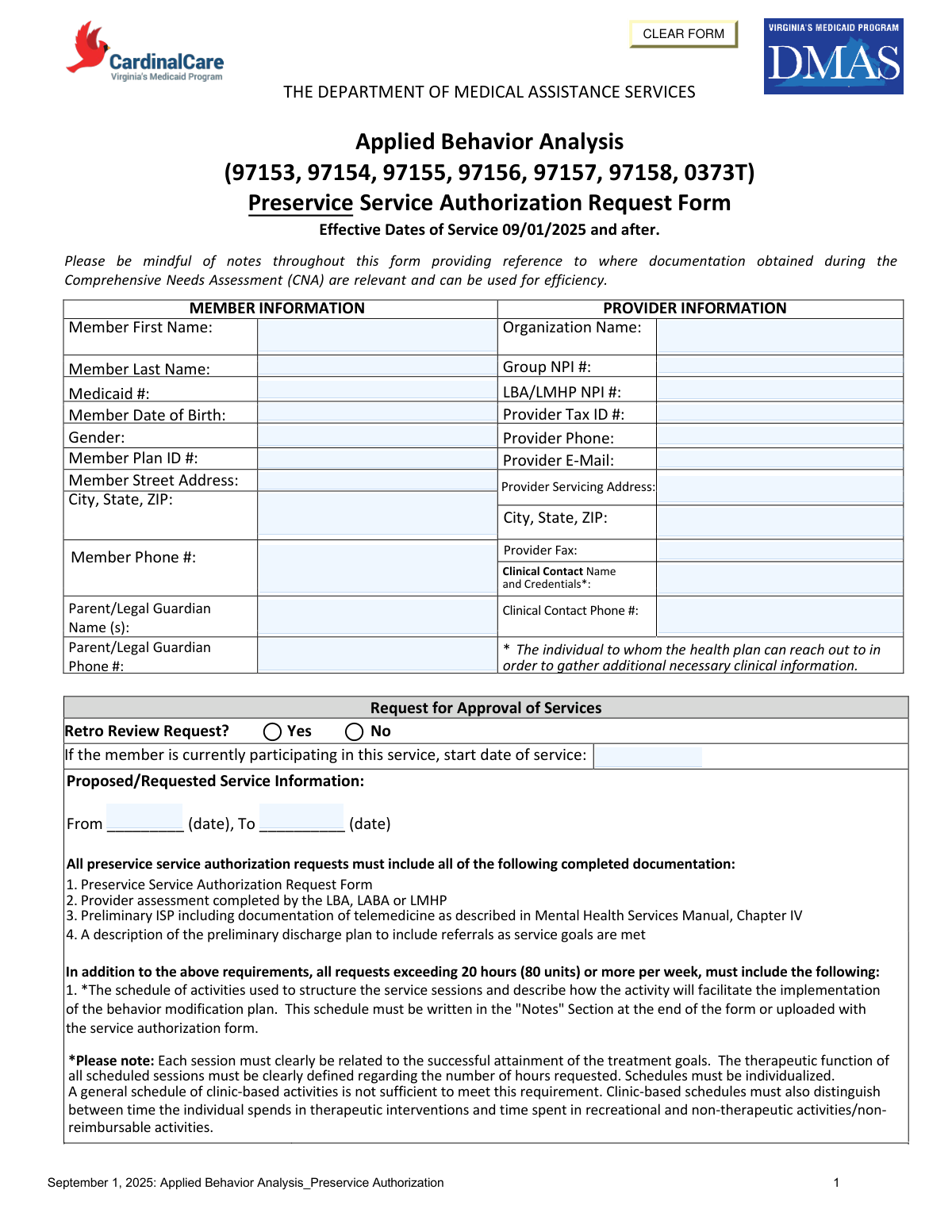
Yes! You can use AI to fill out The Department of Medical Assistance Services Applied Behavior Analysis Preservice Service Authorization Request Form (Effective Dates of Service 09/01/2025 and after)
| Fillable fields | 108 |
| Pages | 8 |
| Fields per page | 14 |
| Sections | 43 |
| Conditional rules | 12 |
| Tables & lists | 2 |
| Instruction pages | — |
| Instafill Form ID | IF-THE-DEPARTMENT-OF-MEDICAL-ASSISTANCE-SERVICES-APPL |
Form specifications
| Form name: | The Department of Medical Assistance Services Applied Behavior Analysis Preservice Service Authorization Request Form (Effective Dates of Service 09/01/2025 and after) |
| Number of fields: | 108 |
| Number of pages: | 8 |
| FCI: | Complex (68/100) |
| Field instructions: | DMAS ABA Preservice Authorization Request Instructions |
| Filled form examples: | DMAS ABA Preservice Authorization Request Examples |
| Language: | English |
Instafill Demo: How to fill out PDF forms in seconds with AI
How to Fill Out DMAS ABA Preservice Authorization Request Online for Free in 2026
- 1 Enter member information (name, Medicaid number, DOB, gender, plan ID, address/phone) and parent/legal guardian contact details.
- 2 Enter provider information (organization name, Group NPI, LBA/LMHP NPI, tax ID, servicing address, phone/fax/email) and identify the clinical contact person and credentials.
- 3 Complete the request for approval section: indicate whether this is a retro review, list current start date if already receiving services, and specify the requested date range (from/to).
- 4 Fill in the proposed/requested service table for each CPT code (97153–97158, 0373T): provider qualifications, daily hours/days per week, total weekly hours, total hours for the requested period, total units requested, and any required notes.
- 5 Document prior ABA/behavior therapy treatment periods in the past 12 months (provider, dates of service, outcomes).
- 6 Complete clinical justification: ICD-10 primary/secondary diagnoses, DSM diagnosis/provisional diagnosis, symptom description and functional impairment, admission criteria checkboxes (2A–2E) with narratives, and preliminary treatment goals including telemedicine vs in-person details and clinical evidence when telemedicine is recommended.
- 7 Finish recovery/discharge planning (progress definition, barriers, supports/resources, anticipated discharge level of care and estimated discharge date), attach required supporting documents (assessment, preliminary ISP, discharge plan, and schedule if requesting 20+ hours/week), and obtain LMHP/LABA attestation signature, printed name, credentials, and date.
Our AI-powered system ensures each field is filled out correctly, reducing errors and saving you time.
Why Choose Instafill.ai for Your Fillable DMAS ABA Preservice Authorization Request Form?
Speed
Complete your DMAS ABA Preservice Authorization Request in as little as 37 seconds.
Up-to-Date
Always use the latest 2026 DMAS ABA Preservice Authorization Request form version.
Cost-effective
No need to hire expensive lawyers.
Accuracy
Our AI performs 10 compliance checks to ensure your form is error-free.
Security
Your personal information is protected with bank-level encryption.
Frequently Asked Questions About DMAS ABA Preservice Authorization Request
DMAS ABA Preservice Authorization Request has a Form Complexity Index of 68 out of 100, placing it in the complex complexity tier. This score is calculated deterministically from the form’s own structure using Instafill’s published Form Complexity Index methodology, so it can be reproduced and independently verified — it is not a subjective estimate.
For DMAS ABA Preservice Authorization Request specifically, the score reflects 108 fillable fields across 8 pages, grouped into 43 sections, and 12 conditional fields that only apply depending on earlier answers, 2 tables or repeating lists. The number of fields is the largest factor in the base score (weighted 36%), followed by how difficult those fields are to complete based on their type, where free-text and signature fields count for more than simple checkboxes (26%). The number of pages that actually contain fields (15%), the amount of conditional “fill-only-if” logic (16%), and how many sections the form is divided into (7%) account for the rest of the base. On top of that base, the index adds points for tables and repeating lists, bundled instruction pages, and dense page layouts — capturing difficulty the base alone can miss.
In practical terms, a complex score means the form is demanding, with many fields, multiple pages and branching rules that are easy to get wrong. Instafill removes that effort entirely: our AI reads your information, maps each value to the correct field — including the conditional ones — and completes DMAS ABA Preservice Authorization Request accurately in under a minute, with every field available for you to review before you download. See exactly how the Form Complexity Index is calculated.
Compliance DMAS ABA Preservice Authorization Request
Validation Checks by Instafill.ai
Common Mistakes in Completing DMAS ABA Preservice Authorization Request
“I was never sure if my IRS forms like W-9 were filled correctly. Now, I can complete the forms accurately without any external help.”
Your data stays secure with advanced protection from Instafill and our subprocessors