Compliance VA Form 29-357
Validation Checks by Instafill.ai
1
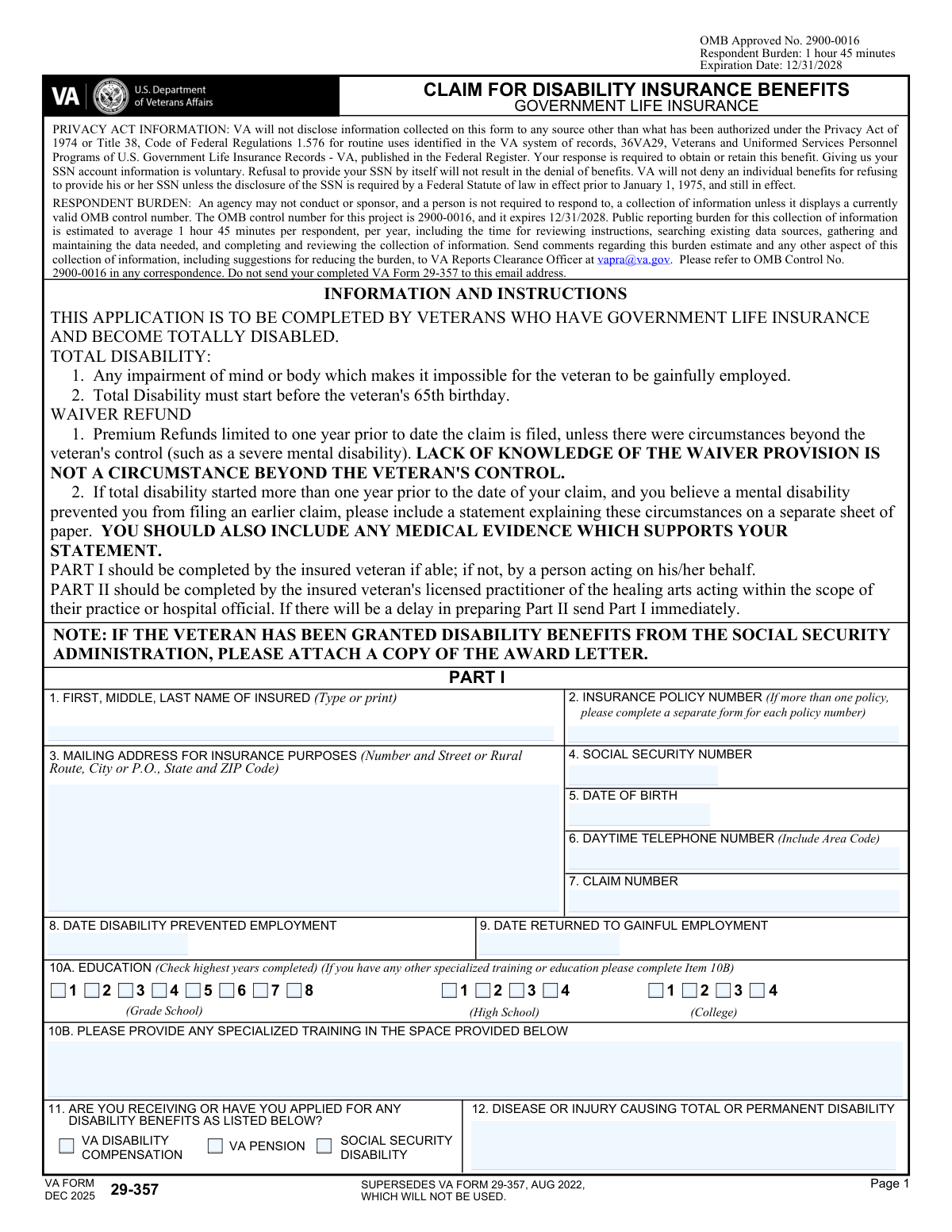
Insured Full Name Completeness and Character Validation
Validates that the insured’s name (first, middle, last) is present and not left blank or entered as initials-only (e.g., “J D”). It should allow common name characters (letters, spaces, hyphens, apostrophes) and reject numeric-only or symbol-heavy entries. This is important for identity matching across VA insurance records and medical documentation. If validation fails, the submission should be flagged for correction because the claim may not be matchable to the correct insured.
2
Insurance Policy Number Format and Single-Policy Rule
Checks that the insurance policy number is provided and matches expected formatting rules (e.g., includes required letter prefix if applicable, preserves dashes/letters, and is not truncated). Also validates that only one policy number is represented per submission, since the form instructs a separate form for each policy. This prevents misrouting and incorrect association of disability waiver decisions to the wrong policy. If validation fails, the system should reject or route to manual review and request a separate submission per policy.
3
Mailing Address Completeness (Street/City/State/ZIP) and ZIP Format
Ensures the mailing address includes street or PO box/rural route, city, state, and ZIP code, and that the ZIP is valid (5 digits or ZIP+4). A complete address is required for official correspondence, premium waiver decisions, and refund communications. Missing or malformed address data can cause returned mail and delays in benefits processing. If validation fails, prompt the user to complete missing components or correct the ZIP format.
4
Social Security Number (SSN) 9-Digit and Disallowed Values Check
Validates that the SSN, if provided, is exactly 9 digits (optionally allowing standard dash formatting) and is not an obviously invalid value (e.g., all zeros, 123456789). Although SSN disclosure is described as voluntary, when supplied it must be usable for identity resolution and record matching. Invalid SSNs can lead to mismatched records or processing errors. If validation fails, the system should request correction or allow submission without SSN only if business rules permit.
5
Date of Birth Format and Age-Based Eligibility (Disability Before 65)
Checks that the date of birth is a valid calendar date and not in the future. Then verifies the rule stated on the form: total disability must start before the veteran’s 65th birthday by comparing DOB to the ‘Date Disability Prevented Employment’ (Item 8). This is critical because claims outside eligibility criteria may be denied. If validation fails, the system should flag the claim as potentially ineligible and require confirmation or supporting explanation before submission.
6
Daytime Telephone Number Format and Minimum Contactability
Validates that the daytime phone number contains a valid number of digits (e.g., 10 digits for US numbers, or E.164-compatible if country code is included) and is not placeholder text. Reliable contact information is needed to resolve missing evidence, clarify employment history, or coordinate medical documentation. Incorrect phone numbers increase processing time and can lead to denial for failure to respond. If validation fails, prompt for a corrected phone number or an alternate contact method if supported.
7
Claim Number Presence and Format Consistency
Ensures the claim number field is not blank and conforms to expected VA claim number patterns (e.g., alphanumeric length constraints, no illegal characters). The claim number is used to associate the submission with an existing VA claim record and correspondence. Incorrect claim numbers can cause misfiling or duplicate claim creation. If validation fails, the system should request correction or route to manual indexing.
8
Disability Onset Date (Item 8) Validity and Not After Signature Date
Validates that the ‘Date Disability Prevented Employment’ is a real date and is not in the future relative to the date of signature/submission. This date is central to determining eligibility, waiver start, and potential premium refund windows. A future onset date indicates data entry error or misunderstanding of the question. If validation fails, block submission until corrected or require an attestation/explanation if the system allows exceptions.
9
Return to Gainful Employment Date (Item 9) Logical Consistency
If a return-to-work date is provided, checks that it is on or after the disability onset date and not before the last day worked in the employment records. This prevents contradictory timelines (e.g., returning to work before disability prevented employment). Consistent dates are necessary to evaluate total disability duration and waiver/refund periods. If validation fails, prompt the user to correct the date or clarify that they have not returned to gainful employment.
10
Education Level Selection: Exactly One Highest Year Completed
Validates that the education section (Item 10A) has exactly one “highest year completed” selection across grade school, high school, and college options, and that mutually exclusive boxes are not simultaneously checked. This ensures the data represents a single highest completed level rather than multiple conflicting levels. Education can be relevant to employability assessments and claim context. If validation fails, require the user to select only one highest year completed.
11
Specialized Training (Item 10B) Conditional Requirement and Minimum Detail
If the applicant indicates specialized training/education beyond the basic highest year completed (or if the workflow explicitly asks for it), validate that Item 10B is not blank and includes minimally useful detail (e.g., training name and provider or dates). This information can support employability and vocational context in disability determinations. Empty or vague entries (e.g., “training”) reduce evidentiary value. If validation fails, prompt for additional details or allow “None” explicitly.
12
Disability Benefits Selection (Item 11) and SSA Award Letter Attachment Prompt
Validates that at least one checkbox is selected if the applicant answers “yes” to receiving/applying for benefits, and that selections are limited to the provided options (VA compensation, VA pension, SSA disability). If Social Security Disability is selected, the system should require an attachment indicator or prompt for the SSA award letter as instructed. This helps corroborate disability status and speeds adjudication. If validation fails, request corrected selections and/or prompt for the missing SSA documentation.
13
Cause of Disability (Item 12) Non-Empty and Not Placeholder Text
Ensures the disease or injury causing total/permanent disability is provided and contains meaningful content (e.g., not “N/A”, “unknown”, or a single character). This field is essential for medical evaluation, matching to practitioner reports, and determining whether the condition aligns with the claimed disability timeline. Missing or non-informative entries can stall medical development. If validation fails, require a brief description or diagnosis statement.
14
Hospitalization Entries: Paired Fields and Admission/Release Date Order
For each hospital listed, validates that name, address, admission date, and release date are provided together (no orphaned dates without facility identification). Also checks that admission date is on/before release date and that both are valid calendar dates. Accurate hospitalization history supports medical evidence gathering and timeline verification. If validation fails, prompt to complete missing fields or correct date ordering.
15
Licensed Practitioner Entries: Required Pairing and Treatment Date Sequence
For each practitioner listed, validates that name and address are present when any treatment dates are entered, and that ‘date treatment began’ is on/before ‘date of last treatment.’ This ensures VA can request records and that the treatment timeline is coherent. Incomplete practitioner information can prevent evidence collection and delay adjudication. If validation fails, require completion of missing practitioner identifiers or correction of date sequences.
16
Employment History Completeness and Numeric Range Checks (Hours/Earnings)
For each employment record provided, validates that employer name/address, occupation, dates (from/to), last day worked, hours worked (weekly), earnings (weekly), and reason for termination are present when the record is used. Hours and earnings must be numeric and within reasonable bounds (e.g., hours 0–168; earnings non-negative), and date ranges must be consistent (from ≤ to; last day worked within the employment period). Employment history is required to evaluate gainful employment and confirm when disability prevented work. If validation fails, the system should flag the specific row and require correction before submission.
17
Signature and Date of Signature Presence and Date Validity
Validates that the insured (or authorized fiduciary/official) signature is present and that the date of signature is a valid date not in the future. The signature certifies truthfulness and authorizes release of information, which is necessary for obtaining medical/employment records. Missing signatures or invalid dates can make the submission legally insufficient and unprocessable. If validation fails, block submission until a valid signature and date are provided.