Compliance CMS-855B
Validation Checks by Instafill.ai
1
Legal Business Name Matches IRS Records and NPI Registration
Validates that the Legal Business Name (LBN) entered in Section 2A1 exactly matches the name on file with the IRS (as confirmed by IRS Form CP-575 or equivalent) and the name used to obtain the National Provider Identifier (NPI) in NPPES. This is critical because CMS requires the LBN, TIN, and NPI to match exactly across both PECOS and NPPES systems. If there is a mismatch, the application will be rejected or delayed, and Medicare billing privileges cannot be established.
2
Tax Identification Number (TIN) Format and Consistency Validation
Validates that the Tax Identification Number (TIN) entered in Section 2A1 follows the correct 9-digit EIN format (XX-XXXXXXX) and is consistent with the TIN used to obtain the NPI in NPPES. The TIN must match IRS records exactly, as any discrepancy between the TIN in PECOS and NPPES will prevent enrollment processing. If the supplier is a sole proprietor using an EIN, supporting IRS documentation (e.g., CP-575) must also be submitted.
3
National Provider Identifier (NPI) Type Validation
Validates that the NPI provided is a Type 2 (Entity/Organization) NPI, as required for all applicants submitting the CMS-855B. Sole proprietors must use a Type 1 (Individual) NPI, while corporations, partnerships, LLCs, and other organizations must use a Type 2 NPI. Submitting an incorrect NPI type will result in application rejection, as the NPI type must align with the organizational structure identified in Section 2A1.
4
Date Format Validation Across All Date Fields
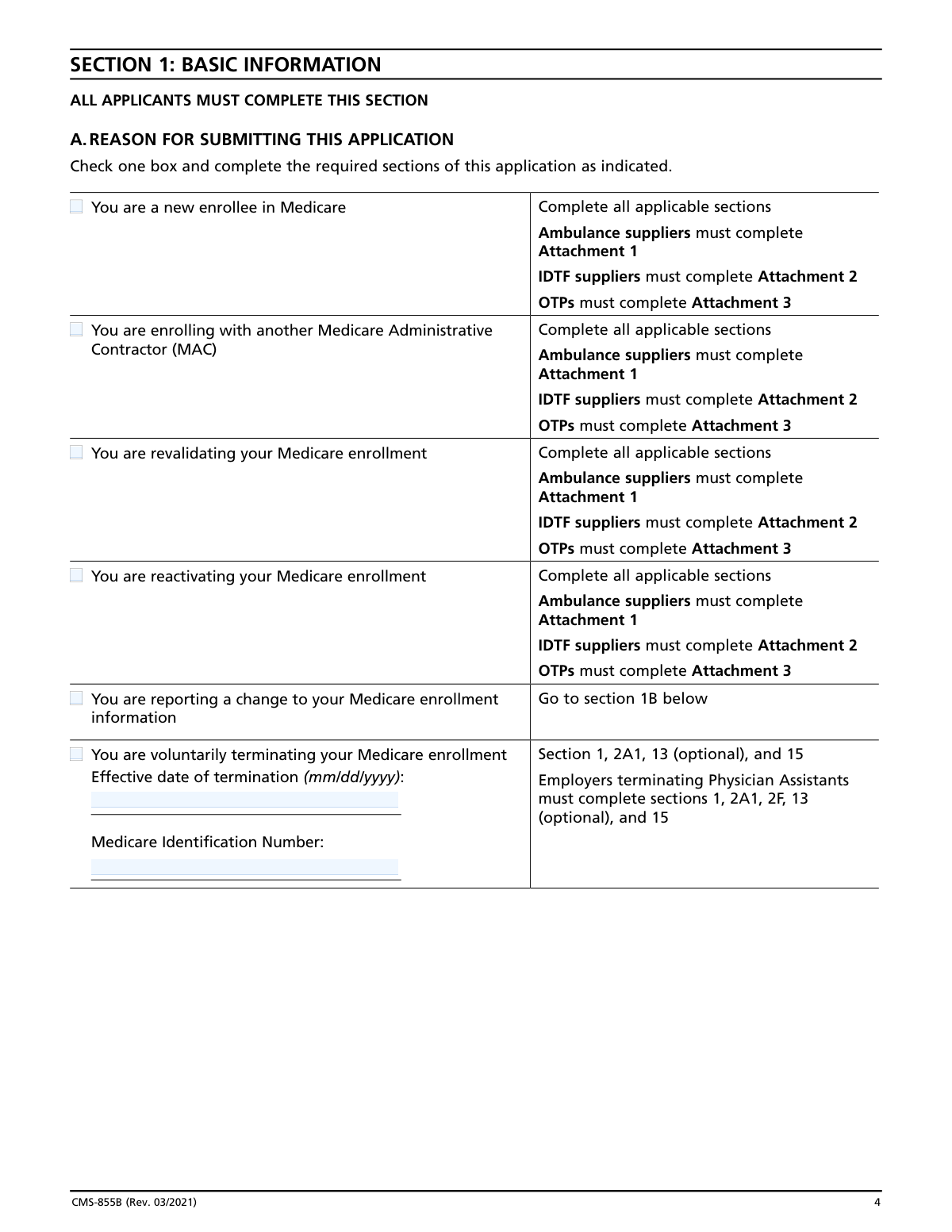
Validates that all date fields throughout the application — including effective dates, dates of birth, license effective/expiration dates, accreditation dates, termination dates, and signature dates — are entered in the required mm/dd/yyyy format. Incorrectly formatted dates are a common cause of application delays and MAC returns. Fields such as the effective date of termination in Section 1, the first Medicare patient date in Section 4A, and all dates in Attachments 1–3 must all conform to this format.
5
Authorized Official Signature and Date Completeness
Validates that Section 15 contains at least one original Authorized Official signature accompanied by a printed name, title/position, telephone number, and a valid signature date in mm/dd/yyyy format. The application explicitly states it cannot be processed without a signature and date. Additionally, the Authorized Official must be reported in Section 6, and their Social Security Number must be disclosed; failure to meet any of these requirements will result in the application being returned unprocessed.
6
Social Security Number (SSN) Format Validation for Individuals
Validates that all SSN fields for individuals reported in Sections 6, 8 (Billing Agent), and Attachments 2 and 3 follow the standard 9-digit format (XXX-XX-XXXX) and are not left blank where required. The form notes that the name, date of birth, and SSN must coincide with the individual's information as listed with the Social Security Administration. Foreign nationals without an SSN must provide an Individual Tax Identification Number (ITIN) instead; submitting an improperly formatted or missing SSN will cause processing delays or rejection.
7
Practice Location Address Cannot Be a P.O. Box
Validates that the Practice Location Street Address entered in Section 4A is a physical street address as recorded by the United States Postal Service and does not contain a P.O. Box. The form explicitly prohibits P.O. Boxes for practice location addresses, as Medicare requires verification of the physical location where services are rendered to beneficiaries. Similarly, the Medical Records Storage Address in Section 4C cannot be a post office box or drop box. Submitting a P.O. Box in these fields will result in application rejection.
8
Correspondence Mailing Address Cannot Be a Billing Agency Address
Validates that the Correspondence Mailing Address provided in Section 2A3 is not the address of a billing agent, billing agency, or medical management company. The form explicitly prohibits this to ensure that official MAC correspondence reaches the supplier directly. Additionally, the billing agency address entered in Section 8 must be verified to differ from the correspondence address in Section 2A3. If these addresses match, the application will be flagged for correction.
9
Reason for Submission Selection and Required Sections Completeness
Validates that exactly one reason for submission is selected in Section 1A (e.g., new enrollee, revalidation, change of information, voluntary termination) and that all sections required for that reason are completed. For example, a voluntary termination requires an effective termination date and Medicare Identification Number, while a new enrollment requires completion of all applicable sections plus relevant attachments (Attachment 1 for ambulance suppliers, Attachment 2 for IDTFs, Attachment 3 for OTPs). Incomplete section coverage based on the selected reason will result in application return.
10
Final Adverse Legal Action History Completeness
Validates that Section 3C is fully completed when a 'Yes' response is given to the question about prior final adverse legal actions, including the specific action, date, and the federal/state agency or court that imposed it. This requirement also applies to organizations reported in Section 5B and individuals reported in Section 6B. All applicable supporting documentation (e.g., notifications, resolutions, reinstatement letters) must be attached. Incomplete adverse legal action disclosures, regardless of expungement or pending appeals, constitute a reportable omission and may result in denial or revocation of billing privileges.
11
Ownership and Managing Control Minimum Reporting Requirements
Validates that the application includes at least one organizational or individual owner (Section 5 or 6), at least one managing employee (Section 6), and at least one Authorized Official (Section 15), as explicitly required by the form instructions. All individuals with 5% or greater direct or indirect ownership, all officers and directors of corporations, all partners, and all managing employees must be reported in Section 6. Missing any of these required disclosures will result in application rejection, as CMS uses this information to assess program integrity risks.
12
License and Certification Effective Date Cannot Be in the Future for Active Licenses
Validates that license and certification effective dates entered in Sections 2A2a and 2A2b are not future dates, as these fields represent currently active credentials. For ambulance suppliers in Attachment 1C, the license effective date must be on or before the date of application submission, and the expiration date must be after the submission date to confirm the license is currently valid. Submitting expired or not-yet-effective licenses will result in the application being returned or denied, as active licensure is a prerequisite for Medicare enrollment.
13
ASC Accreditation Date Logical Consistency
Validates that for Ambulatory Surgical Centers completing Section 2E, the Expiration Date of Current Accreditation is chronologically after the Effective Date of Current Accreditation, and that the expiration date has not already passed at the time of submission. If the ASC is accredited, both dates are required and must form a valid date range. An expired accreditation or a date range where the expiration precedes the effective date indicates an invalid or lapsed accreditation status, which would disqualify the ASC from enrollment.
14
IDTF Supervising Physician General Supervision Site Limit Validation
Validates that each supervising physician listed in Attachment 2E who provides General Supervision is not already providing general supervision at three or more other IDTF sites, as prohibited by 42 C.F.R. section 410.33(b)(1). The 'Other Supervision Sites' table in Attachment 2E must be reviewed to ensure the total number of IDTF sites (including the enrolling facility) does not exceed three for any single supervising physician providing general supervision. Exceeding this limit disqualifies the physician from serving as a supervising physician for the enrolling IDTF.
15
OTP Personnel SSN, NPI, and License Number Completeness
Validates that all Opioid Treatment Program ordering and dispensing personnel reported in Attachment 3A and 3B have complete entries for all required fields: First Name, Last Name, Date of Birth (mm/dd/yyyy), Social Security Number, NPI, License Number, and Practitioner Type. These fields are mandatory for all staff legally authorized to order or dispense controlled substances, regardless of whether they are currently doing so. Missing any of these identifiers for OTP personnel will result in the application being returned, as CMS uses this information to screen against exclusion and preclusion lists.
16
Electronic Funds Transfer (EFT) Authorization Agreement Submission Validation
Validates that a completed CMS-588 Electronic Funds Transfer Authorization Agreement is included with the application for initial enrollments, reactivations, or any changes to banking information, accompanied by a voided check or bank letter. If the supplier has a lending relationship with the bank receiving Medicare payments, a written waiver of the bank's right of offset for Medicare receivables must also be included. Failure to submit the EFT agreement when required will delay the activation of Medicare billing privileges, as routine Medicare payments are made exclusively via electronic funds transfer.